






In the realm of disability care and support, behaviour support practitioners stand out for their unique skills in empowering individuals, …

Understanding and Implementing Positive Solutions Behaviour support is fundamental to providing comprehensive care and assistance to individuals with disabilities. It …
Driving is more than just a way to get from point A to point B; it’s a symbol of independence, …

Embarking on a career in Support Work was a natural step for me, driven by a desire to make a …

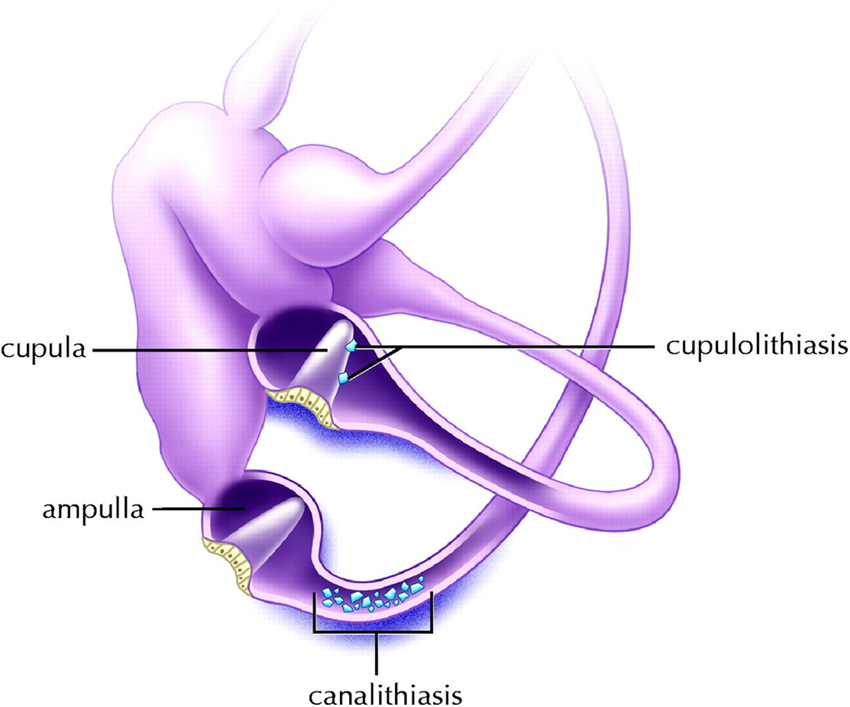
Gaze stability training is a type of exercise utilised in vestibular therapy. Its main aim is to improve the functioning …

Early intervention for children is paramount. It addresses developmental delays or disabilities during infancy and early childhood when the brain …
